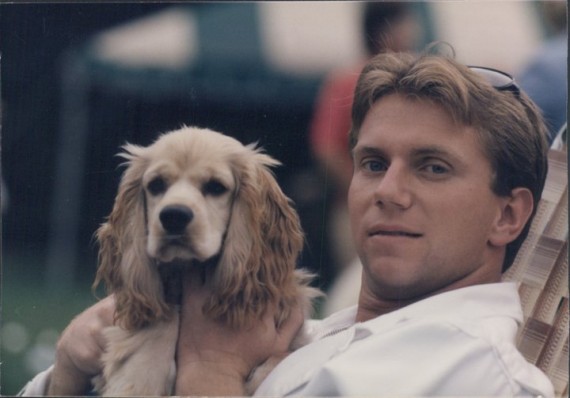
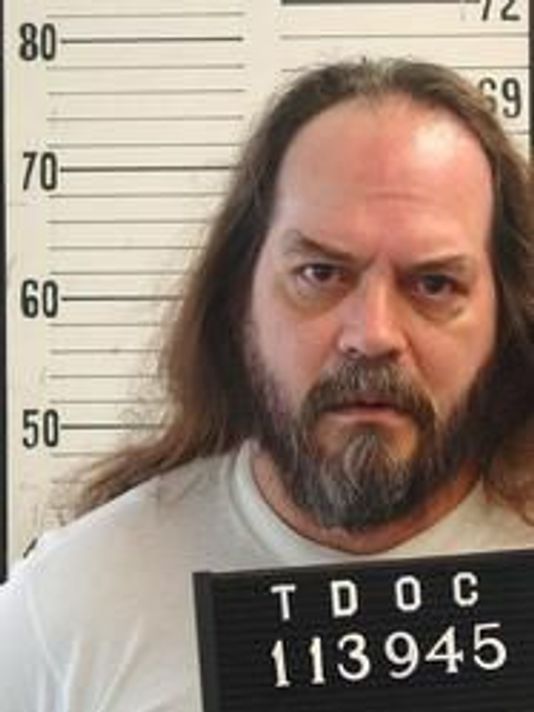
Photos of inmates with mental illnesses who have died in jails. Courtesy Virginia Pilot newspaper
(8-23-18) The Virginian Pilot newspaper has published an extraordinary series – the first ever comprehensive study that tracks deaths of individuals with mental illnesses in jails. It is entitled: Mental illness is a death sentence for many in America’s jails.
Even those of us who are familiar with the inappropriate jailing of Americans who are sick will be shocked by the newspaper’s reporting and the graphics that accompany it. (Please share the series with your local elected leaders.)
Students from Marquette University helped the newspaper track the deaths of 404 inmates with mental illnesses who have died in jails since 2010. They collected information from all 50 states and the District of Columbia.
Here are some headlines from this poignant investigative series:
At least 33 times since 2010, inmates with mental illness have died after their family or friends contacted jails to warn of their loved one’s mental health problems.